
Rejoicing in hope; patient in tribulation; continuing instant in prayer (Romans 12:12)
Dr. Marie D. Kube, Ph.D. and Dr. Michael G. Klug, Ph.D.
Dear Leaders,
This report documents survival and recovery of a severe case of post-traumatic stress disorder, or PTSD, for three years following a nervous breakdown. The purpose of this report is to improve the understanding of PTSD based on expertise and experience which will help to better recognize PTSD, reduce suffering, increase survival and help people with PTSD get better faster.
This report contains the following sections: Introduction, Current Diagnostic Criteria for PTSD, PTSD Physiology, Recognizing PTSD, Surviving PTSD, and Personal PTSD Experience.
Please note that any estimates of amount of time needed to recover from PTSD should not be shared with someone suffering from the condition. While the case described in this report does fit the established time frame that is typically required to retune the brain’s responses, this information can be extremely detrimental to someone with PTSD who cannot bear the condition they are in any longer at all. Further, increasing understanding will lead to decreased suffering.
One contributor to this report, Dr. Marie D. Kube, Ph.D., is also the subject of this case study. Her self-portrait, “PTSD: you can’t do it to yourself,” is the cover picture of this report. She was diagnosed with PTSD at the beginning of 2016, and this diagnosis was confirmed by multiple different medical doctors and other doctors during the following two years. A description of her personal experience is included at the end of this report, and her curriculum vitae (CV) can be read at https://myspiritualconnection.org/2018/01/20/marie-kube-curriculum-vitae/. Another contributor to this report, Dr. Michael G. Klug, is an expert in physiology and his CV can be read at https://myspiritualconnection.org/2018/04/09/michael-klug-curriculum-vitae/ . Drs. Kube and Klug were married for over 20 years and have now been divorced for over two years.

Dr. Michael G. Klug, Ph.D.
Special thanks and acknowledgement to contributors of this work who are not named in this report at this time. This report is to honor you by selflessly passing on to others potentially life-saving information as you also have so selflessly shared.
Introduction
PTSD is a disorder of the nervous system pursuant to traumatic stress, which no one can do to themselves. The brain and nervous system control all bodily functions as well as the interaction of the individual with its environment. Our bodies are not designed to sustain a high level of stress continuously over an extended period.
PTSD is perhaps the most stigmatized mental disorder of all. Even to the medical doctors in the U.S.A. responsible for treating the condition in the emergency rooms, “PTSD” has nothing but negative connotations. It reminds us that the original purpose of American doctors was to return soldiers to the battlefield quickly during war. This is the legacy of a culture rooted in war.
The notion that “I, or someone I know, went through something similar and didn’t develop PTSD, so I don’t understand what your problem is and why you cannot just get over it” is a primary example of detrimental misperceptions about PTSD. Such detrimental misperceptions are being relentlessly spread by those who are responsible for hurting others and then shaming and blaming the victims and kicking them while they are down and encouraging others to do the same. The result is that people with PTSD commit suicide every day now. For all afflicted with PTSD, past and present, this report aims to tell the truth that is good, to the best of our knowledge and experience, in effort to bring about positive change for us all.
Symptoms of trauma-related mental disorders have been documented since at least the time of the ancient Greeks. What is now called “PTSD” has been known previously as “shell shock” and “combat neurosis.” PTSD was erroneously classified as an anxiety disorder until recently but has been reclassified as a “trauma- and stressor-related disorder” in Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition, Published May 18, 2013 (DSM-5).
Current Diagnostic Criteria for PTSD
Diagnosis of PTSD is currently based on the presence of specific symptoms following a traumatic event that were not present before exposure to the traumatic event. The diagnostic criteria for PTSD, stipulated in the International Statistical Classification of Diseases and Related Health Problems 10 (ICD-10), may be summarized as follows:
1) Exposure to a stressful event or situation (either short- or long-lasting) of exceptionally threatening or catastrophic nature, which is likely to cause pervasive distress in almost anyone
2) Persistent remembering or “reliving” the stressor by intrusive flashbacks, vivid memories, recurring dreams, or by experiencing distress when exposed to circumstances resembling or associated with the stressor
3) Actual or preferred avoidance of circumstances resembling or associated with the stressor (not present before the stressor)
4) Either (a) or (b):
a) Inability to recall, either partially or completely, some important aspects of the period of exposure to the stressor
b) Persistent symptoms (for more than a month after the event) of increased psychological sensitivity and arousal (not present before exposure to the stressor) shown by any two of the following:
i) Difficulty in falling or staying asleep
ii) Irritability or outbursts of anger
iii) Difficulty in concentrating
iv) Hyper-vigilance
v) Exaggerated startle response
PTSD should not be diagnosed unless there is evidence that it arose within six months of a traumatic event of exceptional severity such as one that is life-threatening, according to the ICD-10. PTSD should be differentiated from other disorders such as anxiety disorders, obsessive-compulsive disorder, brief psychotic disorder, schizophrenia, major depressive disorder, and drug-induced psychotic disorders. PTSD should also be differentiated from other adjustment disorders resulting from stressor and symptom patterns that do not meet the criteria for PTSD, such as a partner being fired or a spouse leaving, according to the Wikipedia article on Posttraumatic Stress Disorder. In addition to evidence of trauma, there must be repetitive, intrusive recollection or re-enactment of the event in memories, daytime imagery, or dreams.
Malingerers who claim they have PTSD because they believe that they can obtain a financial, legal, and/or social advantage, such as financial support, do so at the expense of those who truly have PTSD.
Most people who have experienced a traumatic event will not develop PTSD. PTSD is caused by experiencing or witnessing a stressor event involving death, serious injury or such threat to the self or others in a situation in which the individual felt intense fear, horror, or powerlessness. People who experience interpersonal trauma such as rape and child abuse are more likely to develop PTSD as compared to people who experience non-assault-based trauma such as accidents and natural disasters. About half of people develop PTSD following rape. Childhood trauma, chronic adversity, domestic violence and familial stressors increase risk for PTSD. Experiencing bullying as a child or an adult has been correlated with the development of PTSD. See Wikipedia article on Posttraumatic Stress Disorder.
Intentional control responses, like suppression, increase the frequency of unwanted intrusive thoughts. Suppression of intrusive thoughts may be important in the development and maintenance of PTSD.
PTSD is not fear; PTSD is beyond fear. PTSD is not an excuse for failure. PTSD is not a sign of weakness or of not being able to handle what others could. PTSD is not drug addiction. PTSD is being the best in the worst. PTSD is an injury that cannot be self-inflicted. And people with PTSD can get better.
There is no fear in love; but perfect love casts out fear: because fear has torment. He that fears is not made perfect in love (1 John 4:18).
Perhaps someday there will be a computer program, or application, to calculate trauma exposure. PTSD could be viewed as a spectrum with differing possible degrees of severity, for example. A PTSD score could be assessed using criteria specific to traumatic stress. For example, a PTSD score could be similar to a “CAPS score” for the clinician-administered PTSD scale for DSM-5 (CAPS-5), except that the PTSD score will be more accurate because it will be independent of invalidating clinicians who have never had PTSD, who have an erroneous understanding of PTSD at best, who are unable to make PTSD better, who make PTSD much worse, and who do not care about people with PTSD unless they can make a lot of money experimenting on treating their symptoms only and not the causes of PTSD. The PTSD score can be a score on a scale of 0-10, for example, where 0 means no PTSD and 10 means the most severe case of PTSD ever known. In addition to diagnostic criteria such as those described above, the PTSD score can take into account physiologic parameters such as blood pressure, heart rate, capillary refill in the fingernail beds, color of the blood and pupil diameter measured under appropriate lighting conditions.
In the case study described here, the subject was first diagnosed with PTSD at a pain clinic in Twin Cities, Minnesota, U.S.A., on March 10, 2016. She was 49 years old. After suffering with a persistent painful Bartholin gland cyst for 20 years, the cyst became so swollen, red and painful that a surgical procedure was required to cut open the gland and suture the edges to make the opening of the gland bigger (marsupialization). The subject and her advocate requested same-day surgery and were referred to an emergency department in Twin Cities, Minnesota on January 10, 2016. But the managed care system prescribed antibiotics for 10 days and the opioid oxycodone tainted with acetaminophen (aka Tylenol) for the pain, which caused liver toxicity and brain damage while waiting for surgery until late in the afternoon on January 19, 2016.
Even Wikipedia has cited evidence that antibiotics do not work for a Bartholin gland cyst, let alone one that has been festering for more than two decades. After more than 20 years, the cyst most likely led to the development of chronic inflammation that would prevent antibiotics from getting into the cyst. In fact, one of the subject’s lymph nodes that the Bartholin gland drains into on one side of the groin area appears to be fibrotic because it remains swollen, but not tender, painful or warm, almost three years after the surgery. After marsupialization of the right Bartholin gland, the subject suffered a nervous breakdown and was first diagnosed with PTSD upon referral to a pain clinic for chronic pain syndrome due also to past vehicular accidents, all of which was greatly exacerbated. See blog post at https://myspiritualassociation.com/2017/10/07/three-centimeter-incision/ for more of the story.
The subject of this case study has numerous predispositions to developing PTSD. She was drugged and raped multiple times, including her first sexual experience at 15 years of age. She was bullied as a child and as an adult, especially for being a German-American citizen and having the first name “Dagmar” until she finally changed it to “Marie” during her divorce. The subject has neck and back injuries from multiple vehicular accidents, including being hit by a speeding car while walking across the street and being hit by two different drunk drivers while driving. In addition, the subject experienced chronic adversity including long-term unemployment and family illness. See her statement of personal experience at the end of this report for a more detailed account.

Music helps when triggered
PTSD Physiology
This case study offers a lot of insight into the physiology of PTSD, especially since the subject herself is an accomplished scientist and her ex-husband and primary caretaker, Dr. Klug, is an expert in physiology. Possible physiological mechanisms underlying PTSD are explained here and different analogies are offered.
PTSD can be thought of like a heart attack or any other organ failure, only it is the nervous system that is damaged in the case of PTSD. The nervous system controls and coordinates all functions of the body. The two anatomical parts of the nervous system are the central nervous system and the peripheral nervous system. The central nervous system consists of the brain and spinal cord, while the peripheral nervous system consists mainly of the nerves that extend from the brain and spinal cord.
The largest part of the human brain is the cerebrum. The cerebrum is divided in the middle to make a right and left hemisphere. The sheet of gray matter covering the cerebrum is called the cerebral cortex. The cerebral cortex is the home of the conscious mind. The cerebral cortex enables people to be aware of themselves and their sensations, to initiate and control voluntary movements, and to communicate, remember, and understand. Association areas integrate diverse information to enable purposeful action.
Both sides of the cerebrum have different functions. It is extremely important that one side is not overloaded as compared to the other. Human bodies were not designed to sustain a high level of stress continuously over an extended period of time. Too much traumatic stress can disrupt the emotional balance of the brain. When the nervous system becomes overwhelmed, then there is a break down in the ability to handle matters and the nervous system kicks into fight-or-flight mode.
Fight-or-flight mode is a state that a person achieves quickly in response to a threatening encounter or perception of a dangerous situation. The body’s motors get revved up for vigorous activity, such as fighting or fleeing. A pounding heart delivers more blood and oxygen to muscles used for fighting or running. Cold, sweaty skin means that blood is being diverted from the skin to more vital organs, like the brain. The lungs take up more oxygen as the body’s consumption of oxygen increases. The liver releases more sugar into the blood to provide for increased energy needs. Pain is suppressed. Temporarily non-essential functions, such as digestion and elimination of feces and urine, are inhibited. The eye pupils become dilated to let in more light, so you can see better. Interestingly, the subject in this case study exhibits one-sided pupil dilation regularly.
The fight-or-flight response is governed by the autonomic nervous system (ANS). The ANS is a subset of the central nervous system (CNS), including parts of the brain stem, spinal cord, hypothalamus, amygdala, and cerebral cortex. Unlike the direct voluntary control by the cerebral cortex, the ANS cannot be consciously controlled, at least not without training, practice, adaptation. The hypothalamus is the main integration and control center of the ANS, while the brain stem seems to have the most direct influence over the ANS.
With PTSD, it is not a matter of developing control, but of changing how you react and recognizing the patterns earlier, so you can stop the (involuntary) response before it over-reacts.
The ANS controls bodily functions such as heart rate, blood pressure, digestion, and urination that are not easily controlled by conscious will. Rather, the ANS operates with some degree of independence (autonomic = self-governing). The ANS has two divisions, the sympathetic and parasympathetic divisions. The two divisions have opposite effects. It is the sympathetic division of the ANS that is responsible for the fight-or-flight response, while the parasympathetic division directs rest-and-digest mode, e.g., resting and digesting food after a meal.
Once the sympathetic division of the ANS kicks in, you are in fight-or-flight mode and conscious control is more and more lost. That is why you are different, and you don’t remember.
A maladaptation hypothesis is that PTSD is the result of a bodily mechanism that evolved for our protection and that did work, since the subject did survive, but that is now a detrimental over-reaction. The body is pre-programmed to do what it needs to do to survive by responding a certain way to a stimulus. That certain way of responding is reinforced because it works because the individual survives. But eventually, reaction to too much of a detrimental stimulus becomes over-reaction that becomes pathologic.
Learning what hot is can serve as an analogy. The first time one burns oneself, one learns to pull away from the flame soon enough to avoid getting burned. If the threat of being burned is relentless enough, then the reflex reaction of pulling away eventually overcompensates. For example, one may nearly smack themselves in the face by over-reacting as more somatic motor neurons are activated and cause more skeletal muscles to contract. Indeed, the whole sympathetic nervous system can be activated involuntarily.
PTSD is like a peripheral defense mechanism, a physiologic response against circumstances, like abuse, which the individual can no longer endure and that must change for the individual to survive. PTSD means reacting to what happened to you.
Another analogy is that PTSD is to the body like engine abuse is to a car. An engine that is abused and neglected will not run as smoothly as the same engine when well cared for. The decreased performance and longevity are due to the abuse and neglect and not to the engine being inherently weak or defective. Any engine that is abused enough will break. Just because an engine is broken does not mean that it cannot be fixed.
The problem is that so-called “triggers” cause involuntary peripheral responses that are physically damaging. Triggers are circumstances resembling or associated with the stressor event(s) that involved death, serious injury or such threat to the self or others in a situation in which the individual felt intense fear, horror, or powerlessness. In this case study, it could take up to a week or more to recover from the involuntary physical responses induced by being triggered significantly. Symptoms included sleeplessness, constipation, depression and hyper-vigilance.
When severely triggered, the subject was unable to walk. When most severely triggered, the subject’s lips turned blue and then she passed out and became completely unconscious. The subject’s normally low heart rate and blood pressure would suggest that the heart stopped or there was severe vasodilation. Lost blood pressure was visible as blue lips and caused the subject to pass out. This paradoxical response is the opposite response to what is expected. The subject’s low blood pressure seems to be some sort of adaptation. Indeed, the subject is in very good physical shape.
The brain must be re-trained to learn how not to over-react when triggered so that social interaction is successful. Please note that any estimates of amount of time needed to recover from PTSD should not be shared with someone suffering from the condition. While the case described in this report does fit the established time frame of two to three years that is typically required to retune the brain’s responses, this information can be extremely detrimental to someone with PTSD who cannot bear the condition they are in any longer at all. Further, increasing understanding will lead to decreased suffering. Currently, however, it can take two to three years to retune the brain’s response to circumstances resembling or associated with a stressor event(s). Currently, that can mean two to three years’ recovery time before being able to work and re-integrate again socially without being triggered all the time. The average life expectancy with PTSD is 12 years. Clearly there is much room for improvement, especially given that the subject in this case study has survived and recovered from a severe case of PTSD for over 30 years.
An integral part of PTSD is the fight-or-flight response that is governed by the autonomic nervous system (ANS). The ANS is not easily subjected to voluntary control, which explains why PTSD is not something that someone can do to themselves. Further, activities like dance can help switch from fight-or-flight mode into rest-and-digest mode.
The fight-or-flight response is enhanced by secretion of the amine hormones epinephrine (adrenaline) and norepinephrine (noradrenaline) into the blood by the adrenal medulla. We hypothesize that there is peripheral feedback to the central nervous system in PTSD. For example, signal molecules or messengers such as peptides, proteins, hormones or chemical compounds may be sent from the periphery to the brain, e.g., hypothalamus.
The peripheral feedback hypothesis is supported by the heightened startle response characteristic of PTSD. The startle response tightens muscles and makes you tense as the muscle and joint stretch receptors are activated. The startle response puts you on a higher overall level of alertness. Conversely, pleasurable stimuli bring the overall level of alertness down, pointing to the reticular activating system (RAS). For example, a hot bath alleviates PTSD symptoms almost instantaneously by relaxing the muscles, thereby undoing the startle response. Especially for people with heightened startle response, physical activities, such as dancing and yoga, are essential to relieve the tension.

Hot bath alleviates PTSD symptoms
In the subject of this case study, the erector spinae muscles become tight enough to flatten the back so that the natural curvature of the spine is lost. Tightening of the erector spinae group of muscles pulls on the meninges (membranes covering the central nervous system (brain and spinal cord)) and is transmitted as a physical signal from the periphery to areas of the central nervous system connected to any of the affected meninges. The higher the state of arousal of the subject, the tighter the erector spinae and other muscles become. Feedback from erector spinae muscles to the central nervous system via the meninges is an example of the peripheral feedback hypothesis. Tightening of the erector spinae muscles is another example of an involuntary peripheral response associated with PTSD.

Natural curvature of spine lost in PTSD
In the subject of this case study, hormone(s) regulated by the hypothalamic-pituitary-adrenal axis and ovaries make(s) PTSD worse by lowering the threshold for being triggered. Women can synchronize their hormonal cycles to the moon cycle. A hormone(s) that is tied to the ovarian cycle and synchronized with the lunar cycle, at least in the subject of this case study, changes the trigger point and how severely the subject is triggered. Measuring the time-course of hormone levels during the lunar cycle could identify hormone(s) coinciding with the lunar cycle and having an effect on PTSD. For example, follicle-stimulating hormone, luteinizing hormone, and/or estrogen are candidates. Cortisol is known to show up in stress but does not appear to cycle. Hormone replacement therapy and even birth control pills could influence PTSD and could make PTSD even worse. Similarly, hormones are bound to play a role in PTSD in men as well. PTSD is not purely hormonal, however, since the subject in this case study was triggered, often severely, every day for about the first year following the nervous breakdown, before the start of menopause.
PTSD physiology may suggest that treatment with a class of medications known as beta blockers could be effective. Beta blockers are widely used to treat high blood pressure. Beta blockers are competitive antagonists that block receptor sites for the endogenous catecholamines epinephrine (adrenaline) and norepinephrine (noradrenaline) on adrenergic beta receptors of the sympathetic nervous system that mediates the fight-or-flight response. Some beta blockers are selective for one of the three known types of beta receptors while others block all types of beta-adrenergic receptors. See Wikipedia’s article entitled, “Beta blocker.”
The beta blocker propranolol is a non-selective synthetic beta blocker that blocks both beta 1- and beta 2-adrenergic receptors and crosses the blood-brain barrier. Propranolol has been studied extensively and has been reported to work short-term in reducing PTSD symptoms. But is it really a good idea to treat (suppress) symptoms while invalidating the underlying cause? This is especially concerning given that intentional control responses, like suppression, may be important in the development and maintenance of PTSD. While beta blockers like propranolol may be useful in the short-term, they may actually make PTSD worse in the long-term by maintaining PTSD instead of getting it out.
Why was propranolol chosen for study instead of other beta blockers? Due to the high penetration across the blood-brain barrier, lipophilic beta blockers, such as propranolol and metoprolol, are more likely than other less lipophilic beta blockers to cause sleep disturbances, such as insomnia, vivid dreams and nightmares (Cruickshank JM, 2010, Indian Heart Journal, 62(2): 101, PMID 21180298). Propranolol may therefore be contraindicated for PTSD given that the diagnostic criteria for PTSD described above include “persistent remembering or “reliving” the stressor by intrusive flashbacks, vivid memories, recurring dreams…” and “difficulty in falling or staying asleep.”
Propranolol is used to treat high blood pressure and other conditions, including performance anxiety. PTSD is not an anxiety disorder as was thought until recently when it was re-classified as a trauma- and stressor-related disorder in DSM-5. In this case study, the subject’s normally low blood pressure may contraindicate treatment with beta blockers. For example, after a one mile walk to the pharmacy, the subject’s systolic pressure was 93 mmHg, diastolic pressure was 53 mmHg, and pulse rate was 58 beats per minute.
Memory disruption by noradrenergic receptor antagonism during memory reconsolidation after reactivation/retrieval using propranolol has been researched widely in humans for the treatment of neuropsychiatric disorders such as PTSD. “Forgetting therapy” is unethical according to Beyond Therapy, a report published by the President’s Council on Bioethics (US) (2003). The major argument made against “forgetting therapy” is that it is unethical as “our happiness depends also on our memory, on knowing who we have been” (President’s Council on Bioethics (US), 2003, p. 209). Nevertheless, propranolol has been widely used in attempt to specifically wipe out bad memories that cause emotional problems without making patients forget all their life experiences as well.
There are more than 20 human trials of propranolol for PTSD listed in ClinicalTrials.gov (a service of the U.S. National Institutes of Health), including 4 trials that were terminated for low enrollment, for example. No wonder the numbers of patients studied are often too small to be meaningful. Conventional follow-up time periods for PTSD clinical trials are only 3, 6, or 9 months. One 2012 study claiming that treatment with propranolol is associated with better quality of life among PTSD patients had study participants that met the DSM-IV criteria for chronic PTSD. As noted above, PTSD has been reclassified as a “trauma- and stressor-related disorder” in DSM-5, published 2013. Furthermore, the study was only 5 months from pre-treatment to follow-up and only had 33 participants (Poundja et al., 2012, European Journal of Psychotraumatology, 3: 15470). The participants were not even seeking treatment when enrolled in the study. The paper concludes that, “These results must await publication of a randomized-controlled trial to further delineate effectiveness with the novel treatment approach.” Where are the results of the trial? A 2018 publication about a 6-week trial of propranolol in 60 adults diagnosed with “long-standing PTSD” concludes that “Replication studies using a long-term follow-up in various trauma populations are required (Brunet et al., 2018, Am J Psychiatry, 175(5):427, PMID: 29325446). Continued exposure to propranolol may be necessary for long-term benefits and may lead to desensitization. Results are expected in May 2019 for a trial with 40 participants suffering from “betrayal or abandonment by a significant other during times of need,” but not people suffering from PTSD.
This is brainwashing! Why are psychiatrists and not physiologists studying PTSD? Why is PTSD being treated as psychosomatic when the physiology is somatopsychic?
We predict that a peripherally active beta blocker that does not cross the blood-brain barrier would show an effect in PTSD patients where propranolol is effective. Switching from a centrally to a peripherally acting beta blocker may even work better provided that the beta blocker is not contraindicated.
The Committee on Treatment of Posttraumatic Stress Disorder (2008) found the evidence for all classes of drugs reviewed (alpha-adrenergic blockers, anticonvulsants, novel antipsychotic medications, benzodiazepines, MAOIs, SSRIs, and other antidepressants) inadequate to determine efficacy for patients with PTSD (Institute of Medicine. 2008. Treatment of Posttraumatic Stress Disorder: An Assessment of the Evidence. Washington, DC: The National Academies Press. https://doi.org/10.17226/11955.)
In the most comprehensive set of meta-analyses (2016) comparing psychotherapy and medication efficacy for PTSD, trauma-focused psychotherapies resulted in greater sustained benefit over time by every measure considered as compared to medications: aripiprazole, brofaromine, bupropion, citalopram, divalproex, fluoxetine, guanfacine, mirtazapine, nefazodone, olanzapine, paroxetine, prazosin, risperidone, sertraline, tiagabine, topiramate, and venlafaxine (Lee et al., 2016, Depression and Anxiety 33:792). Interestingly, propranolol was used in the search terms for the meta-analysis but did not meet the inclusion criteria for the study.
Why have so many other drugs been studied for PTSD when the plant called marijuana actually works? There are only 6 trials listed for marijuana in ClinicalTrials.gov, 2 of which are really CBD trials and one of which includes propranolol as a control! The answer is conflict of interest. For example, thirty-one of the medication trials (72%) were industry supported in the most comprehensive set of meta-analyses comparing psychotherapy and medication efficacy for PTSD (Lee et al., 2016, Depression and Anxiety 33:792). Picture white male doctors taking propranolol to steady their hands during surgery or to overcome their performance anxiety. Now picture African American men smoking marijuana after the Vietnam War and current traumatic events. The white men are honored while the black men are imprisoned.
Think of the hundreds of millions, perhaps even billions, of taxpayer dollars, that, instead of going to people with PTSD, have gone to: medical doctors, clinical trials, preclinical research, drug companies, universities, psychiatrists, psychologists, medical writers, publishers, none of which has helped people with PTSD in the long term.
Recognizing PTSD
Together with diagnostic criteria such as the ICD-10 criteria summarized above, outward signs of PTSD can help to identify and treat people with PTSD better. Recognizing signs of PTSD can improve accuracy and speed of diagnosis which, in turn, should improve prognosis as affected people are identified and helped more efficiently and effectively. Major signs and symptoms believed to be associated with PTSD based on this case study are detailed below. More data from others affected with PTSD will determine the general applicability of the signs and symptoms described herein that are based on our experience and that are consistent with our current physiological understanding of PTSD.
People with PTSD go to great lengths to avoid their triggers, and social withdrawal is a hallmark of PTSD. The subject of this case study lacks a social support system. She was triggered more than supported for the first year following her nervous breakdown. She was very depressed, often crying and even suicidal. She was highly reactive and prone to emotional outbursts. She lost trust completely. She withdrew further socially. She avoided eye contact. She moved away to where she did not know anyone, and she lived alone. Her startle response is still heightened after almost three years.
People with PTSD have difficulty sleeping. The nightmares can be intense. The subject in this case had severe sleep disturbance for the first year following a nervous breakdown, during which time she slept less than or equal to three hours a night. Sleeplessness was often accompanied by intense night sweats that soaked the bed, the covers and even a towel. These symptoms were further complicated by the onset of menopause around the middle of the three-year recovery period. After almost three years of recovery, the subject sleeps much better overall but still suffers from significant sleep disturbance due to unwanted and intrusive memories and lingering night sweats.

Night sweats
An underlying neuropathy remaining in the subject’s left upper back after a vehicular accident about 15 years ago caused by a drunk driver is somehow also linked to the sweating outbreaks. For example, after an enormous release (pop) of the muscle in the affected area with exercise, hot bath, and massage, the subject broke out in a sweat that started at the site of the pop and radiated progressively outward form it. The sweat was profuse enough to soak through a large towel into the sheets and mattress of the bed.
PTSD fight-or-flight mode slows down anal elimination. The body shuts down elimination in preparation to fight or to flee. Either way, it is not a good time for a bowel movement. But what is present as a natural coping mechanism in case of a rare event becomes life threatening in abnormal situations. When what should be a rare event is a constant and severe threat that cannot be escaped or relieved sufficiently, then one can become trapped in fight-or-flight mode. Remaining in fight-or-flight mode for extended periods of time is known to have an overall taxing effect on the body that results in significantly decreased life expectancy. Being in fight-or-flight mode too much and/or for too long can cause anal retention so severe that it is life-threatening. Staying in fight-or-flight mode can also burn a lot of calories, especially sugar.
Even with optimal diet and exercise and avoidance of triggers, a baseline state of fight-or-flight mode can cause net retention of feces backed up throughout the voluminous lengths of intestines until the entire abdomen is hard and painfully swollen. This can happen even if some feces, but not enough, are eliminated every day. Night sweats and dehydration make it much worse. It is important to drink a lot of water and to eat a healthy diet. In the subject of this case study, even drinking more than a gallon of water every day could not prevent PTSD-induced constipation. The subject was very hydrated as evidenced by frequent urination about every hour during the day and at least once or twice during the night, yet PTSD-induced constipation was still an issue. Long walks every day are very helpful. See more below under “Surviving PTSD.”
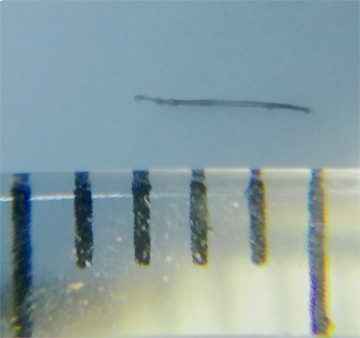
Based on the “hook” shape of the feces, they appear to be getting stuck in the sigmoid colon and assuming that shape. The feces can be so large and hard that they must be thrown in the trash because they cannot be flushed down any toilet. The feces can be hard as a brick, very compacted and dried, like with opioid-induced constipation. This may indicate a link to the opioid system in the gastrointestinal tract. However, the opioid oxycodone had no effect on PTSD symptoms, indicating it works by a different pathway. Even if morphine does not work directly on PTSD symptoms, it is still needed for surgery.
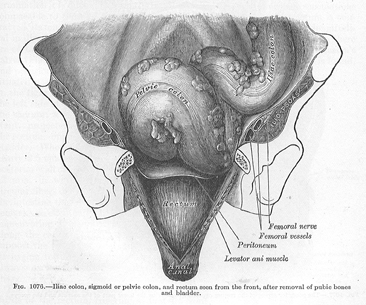
Sigmoid colon has an “S” shape

Stuck feces #1
Stuck feces #2

Stuck feces #3
When triggering of the PTSD finally ends and the body finally shifts from fight-or-flight mode into res-and-digest mode, then the transverse colon may dump a lot of feces at once. For example, one to two feet of feces can be excreted at one time in one very long stool. It may be necessary to relieve oneself multiple times in one day when the release finally happens.
Being more sensitive to cold than heat is a sign of PTSD. This is because exposure to cold triggers the sympathetic division of the autonomic nervous system. People with PTSD also seem to be thin, consistent with the energetically taxing state of remaining in fight-or-flight mode.
Emotional trauma caused by physical violations can cause dissociation and splitting of the consciousness as a coping mechanism. Any sexual abuse, such as rape or incest, usually causes fragmentation of the personality. The experience of the trauma is stored in a fragment of the consciousness that becomes separated and isolated from the main consciousness or personality. Severe fragmentation comes with intense emotional residue. See Spirit Releasement Therapy by William J. Baldwin, D.D.S., Ph.D., 2012, Headline Books, Terra Alta, WV, http://www.HeadlineBooks.com . Treatment involves identification and integration of the fragment(s). We hold onto trauma. The emotional and physical residues of trauma must both be resolved in order to recover from the trauma fully.
It is hypothesized that signs of PTSD, if severe enough, could be manifested on the body’s largest organ, the skin. There are nerves in the skin and PTSD is damage to the nervous system which may, therefore, be visible in the skin.
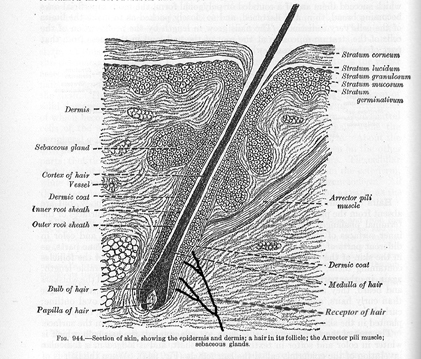
Hair root in skin with innervation by receptor of hair
In the case described here, the subject’s skin has had acne and blemishes since puberty, especially on the face. One infection under the right eye was serious enough to necessitate antibiotics and time off from work. The subject has also had regular outbreaks of unexplained hives for more than 15 years (urticaria, likely stress-induced). In addition, the subject has a propensity to develop ingrown hairs.
PTSD causes nerve damage. Underlying nerve damage, especially when coupled with scarring and other harm such as shaving, waxing or plucking, can lead to inflammation. Indeed, physiologic processes have been discovered linking the immune system and the nervous system. For example, white blood cells express beta 2-adrenergic receptors making them sensitive to changes in autonomic nervous system output (Bruynzeel PL, 1984, Eur. J. Respir. Dis. Suppl., 135:62). Swelling associated with inflammation of the skin can make it difficult or impossible for new hairs to grow through the skin, instead trapping them and causing them to grow in the skin instead of out of the skin.
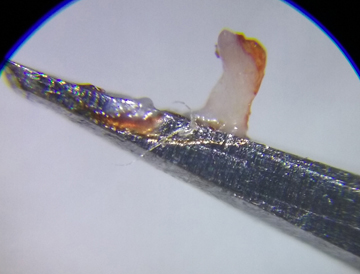
The ends of many extracted hairs from the subject that were ingrown for a long time appeared split under magnification. It is unclear whether split ends are a cause or effect of ingrown hairs. Scars seem to block hairs from growing out of the skin, making them ingrown and possibly causing the ends of the hairs to split as they become more ingrown. Scars can also contain hairs and follicles that were trapped when the open wound in the skin was sewn closed with stitches and healed over. Scars may also cause ingrown hairs, e.g., by causing inflammation and/or by causing fibrosis and death of hair follicles.
Ingrown hair with split end
Ingrown hairs eventually can become partially degraded and the follicles can become fibrotic because the body tries to break them down because they are abnormal and causing damage. For example, as hairs become more and more ingrown, the hair follicle may die and become fibrotic. It may also be that fibrosis of the ingrown hair follicle precedes death in addition to or instead of the other way around. It is also possible that nerve damage underlying PTSD causes, or predisposes to, death and then fibrosis of hair follicles and/or fibrosis and then death of hair follicles. For example, a chronic sympathetic nerve signal to the hair follicle could cause death and fibrosis of the follicle, which causes inflammation and ingrown hairs. It does not seem likely that inflammation itself is the cause of fibrosis and death of the hair follicles because the hairs are several millimeters long, indicating that they grew despite the inflammation.
Hair is made of protein that is incredibly stable. Ingrown hairs can, therefore, persist for a long time and cause a vicious cycle of inflammation which, in turn, can cause more ingrown hairs and scarring in a self-perpetuating cycle that continues until the inflammation is gone. Thick skin and fast healing skin and dermis can make it harder for hairs to grow out through the skin, as in this case, thereby exacerbating the problem of ingrown hairs.
The ingrown hair problem in this case was bilateral. For example, both sides of the face in the areas above the corners of the mouth would have an ingrown hair in about the same position at about the same time. The bilateral nature of ingrown hairs in this case of PTSD is evidence that the nerve damage underlying PTSD exacerbates the problem of ingrown hairs. The subject has also exhibited bilateral pustules. For example, a pustule appeared on the left upper arm at the end of November that was swollen full of pus and blood so that it protruded about a quarter of an inch above the surface of the skin. Then on the next day, a similar pustule appeared in a similar location on the right upper arm.
People with PTSD should avoid shaving, waxing, plucking or tweezing to remove hair. It is best to just trim unwanted hairs with scissors made for cutting hair. Scars may require special attention as they may contain trapped ingrown hairs, and scars may cause ingrown hairs by preventing them from growing out through the skin. Any cause or potential cause of inflammation of the skin should be avoided, if possible, and, if not, treated with special caution (e.g., tattooing, piercing, makeup and perfumes).
Numerous ingrown hairs and fibrotic hair follicles were removed from different affected areas of the subject’s body including the scarred chin, the area between the chin and lower lip, the areas above the left and right corners of the mouth, and the vaginal labia. The ingrown hairs were typically about 1-2 mm in length, but some were 3 mm in length or longer, especially in and around the scar on the chin. Samples were saved for future analysis, e.g., electron microscopy. For years following the subject’s nervous breakdown, as many as 10 ingrown hairs a day were removed from areas that had festered for possibly years and even decades judging by how degraded they were and how putrid they smelled.
3 mm ingrown hair

Fibrotic ingrown hair 60X magnification

Fibrotic ingrown hair bulb 100X magnification

Nonfibrotic ingrown hair bulb 100X magnification
Several scars around the mouth would indicate that the subject was “bitch slapped” or punched in the face on the right and left sides of the mouth as well as below the mouth. The canine tooth pierced through the skin on each side of the mouth leaving scars from the puncture wounds above the corners of the mouth. Four lower teeth appear to have pierced through the skin between the lower lip and chin. The wound was closed with many sutures leaving a couple of irregular scars about an inch long.
Sutures must have a high enough tensile strength to hold skin together until it can grow back together to close the wound. Natural products like silk, cotton and catgut were used until the 1940s. Nylon and Dacron were the first synthetic materials made into sutures, and then polyethylene, polypropylene, polyglycolic acid (Dexon), and polyglactin 910 (Vicryl). Sutures are divided into two groups, absorbable and nonabsorbable.
In the subject of this case study, “absorbable” sutures were not absorbed completely and should never have been used on the face. The body reacted to the sutures, and/or fragments thereof, as foreign bodies that do not belong. The reaction of the body is to try and rid itself of the invader. The foreign body reaction is an inflammatory response that results when immune cells of the body called macrophages are unable to destroy foreign substances that have entered or invaded body tissues. Large numbers of macrophages surround and enclose the target. Other immune cells and fibroblasts surround the macrophages. The resulting granulomas are common in foreign body reactions.
Some parts or segments of the sutures remained and rotted for decades in the subject’s face. The absorbability of “absorbable” sutures depends on factors including age, location (e.g., face), ratio of adipose to muscle tissue and nerves. The face is not a good place to use these sutures, especially since the skin heals quickly to wall off the foreign objects. Pieces of collagenous-looking, incompletely dissolved sutures were extracted from the subject’s face, and samples were saved for future analysis, e.g., gas chromatography – mass spectrometry.
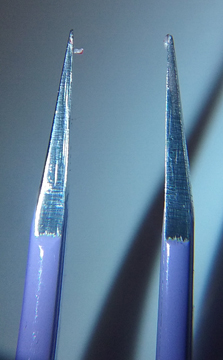
Suture fragment on forceps at 60X magnification
Suture fragment on forceps showing bend at 100X magnification

Suture fragment #2 on end of forceps showing bend at 100X magnification
It appears from the extracted pieces that the “absorbable” sutures were more like little pieces of suture material linked together with dissolvable linkers. But in reality, absorbable sutures made from synthetic polymers are melted and extruded into fine fibers that are then braided into sutures. At least in the subject’s case, fragments of suture material appeared to have been encapsulated as foreign bodies instead of being “absorbed” by the body as intended.
Following removal of putrid ingrown hairs and unabsorbed fragments of “absorbable” stitches from the face of the subject of this case study, there was typically a rash around the affected area, on the forehead, and often the same side of the face. Lesions could even appear on the same side of the neck and abdomen or the entire face and torso. A decreased threshold for being triggered after removal of these stitches in the subject of this case study once again indicates that a peripheral sensory feedback to the ANS is involved in PTSD. Perhaps there is even a linkage between the site of physical injury and the regulator of the sympathetic responsiveness. Such a regulator could be a particular part of the CNS, for example.
Surviving PTSD
The single most important treatment for PTSD, especially PTSD-induced constipation, is drinking lots of clean water and eating a healthy, gluten-free, high-fiber diet of whole foods, preferably organic foods, such as oats, beans, greens (e.g., spinach and cabbage), squash, onions, potatoes, sweet potatoes, corn, quinoa, vegetables and root vegetables, fruits, and seafood (e.g., wild caught fish and crab legs). For example, eat nuts instead of gummy bears if there are no allergies to the nuts. Probiotics may also help.
See the diet recommended by Dr. Terry Willard, Ph.D., Clinical Herbalist, as part of the Wild Rose Herbal D-Tox 12-Day cleanse (https://www.gardenoflife.com/content/product/wild-rose-herbal-d-tox/ ). For more advice about living a healthy lifestyle for at least half a century, see Sexiest at 50: PTSD PhD Marie (available at https://www.amazon.com/Dr-Marie-D-Kube-PhD/e/B07GTTMP1B and https://myspiritualconnection.org/2018/08/18/the-book-beat-bookstore/ and https://myspiritualassociation.com/2018/08/18/quimbys-bookstore/ ).
Let your food be your medicine, and let your medicine be your food, said Hippocrates, the father of medicine.
See an Herbalist, preferably with experience helping people with PTSD, for herbal therapy that is specific and safe for you considering your health status and history. An experienced Herbalist should also be consulted about things like the amounts of herbal medicines to take, the length of time to take them, and what can and cannot be taken together. Also, beware that any given dosage may need to be adjusted based on the potency of the herbal preparation.
In this case study, herbs that helped to overcome more than two years of PTSD-induced constipation were slippery elm bark and marshmallow root. The marshmallow makes the feces take up water, bulk up and be softer, while the slippery elm bark heals hemorrhoids and mucous membranes and makes everything slide out easier. During constipation, waste that the body is trying to eliminate can get stuck in the intestines and cause inflammation. This makes it stickier and harder for more waste to get through. An herbal cleanse program seemed to help significantly in conjunction with drinking a lot of water (more than a gallon) every day and eating a healthy diet as described above. It is important to avoid eating flours of grains as they create an elimination problem. Try sprouted corn tortillas, for example, to experience the live grain difference.
Despite following a proper diet, drinking more than one gallon of water every day, exercising and taking herbal remedies, PTSD-induced constipation was still an issue following intensive triggers in this case study. When stool softeners, laxatives, and enemas did not work, then it was at times necessary to physically remove the feces from the anus using a gloved hand with a little Vaseline on the fingers. It can be easier in a bathtub full of warm water with Epsom salts, but the cleanup can be messy. Overuse of stool softeners, laxatives and enemas can be detrimental.
Bee balm tincture, garden sage tea and cooling foods like strawberries, cucumbers, mint and cantaloupe helped to alleviate PTSD-induced night sweats, especially when complicated with menopause in this case. Coral calcium was taken along with vitamin D3 and magnesium malate. Yarrow salve and salves containing comfrey, milky stage oats and sage were used to heal the skin, especially the face (see your Herbalist). Arnica massage oil was used to alleviate back and neck pain (beware that arnica can be toxic; see your Herbalist).
Medical marijuana was necessary in this case for pain, nausea, sleeplessness, depression and other symptoms of PTSD. It can take a large amount of marijuana to break the sympathetic response (see PTSD Physiology above). People with PTSD need to be able to grow their own medicines. The subject in this case study moved to Colorado and Nevada to obtain the life-saving medicine she needed. After sleeping three hours a night or less for about a year, the transdermal cannabinol (CBN) patch (www.MarysMedicinals.com) broke the pattern of sleeplessness, and the subject achieved six and eventually even eight hours or more of sleep per night. CBN is a cannabinoid, a compound in cannabis, that results from the degradation of tetrahydrocannabinol (THC). CBN has deep relaxing properties that support sleep by allowing your body to fall into a deeper and more restful stage of sleep known as the rapid eye movement (REM) stage. Not only the body, but also the mind is relaxed in the REM state. Quality sleep is known to play a critical role in health.
Transdermal CBN patch for sleeping
In addition to externally applied patches and flowers that can be smoked, medical marijuana is available in many more forms such as edibles, tinctures, capsules, topicals, concentrates. See The Leafly Guide to Cannabis, A Handbook for the Modern Consumer, the Leafly Team, 2017, Twelve, Hachette Book Group, New York, NY, twelvebooks.com. Cannabis-infused coconut oil was like a miracle cure for PTSD-induced constipation (see more in Personal PTSD Experience below) along with slippery elm bark and marshmallow root as described above.
Chiropractic treatment, massage and physical therapy were also critical to survival and recovery in this case. Techniques such as brain re-training were used. Quantum Neuro Reset Therapy, a method of balancing the brain to resolve the emotional shocks, was used (www.qnrt.com). Brain wave entrainment, a process of adjusting the brainwaves to a desired frequency, was also used (www.truerife.com). For example, if a person is in high alert, a stimulus such as pulsed flashing lights or audio tones can be applied to the brain for some time to change the brain frequency towards the applied stimulus and cause a relaxing effect.
Moderate exercise daily is essential to destress. Exercise should have low impact on the joints (e.g., walking, hiking, bicycling, swimming, and dancing). Music, nice people who are validating, and not invalidating, and plans to look forward to are imperative.
Mezcal works for pain, but like all alcohol should only be used in moderation, and only if you and your liver can handle it. MDMA (the active ingredient of ecstasy 3,4-methylenedioxy-N-methylamphetamine) and ayahuasca are more possibilities, although not used in this case. Nitrous oxide may help to relax, especially during dental work.
Personal PTSD Experience
An author of this report, Dr. Marie D. Kube, Ph.D., is also the research subject in the case study described herein. A description of Dr. Kube’s personal experience follows.
My story is a tragedy and a miracle. Despite all my achievements, including having achieved the highest level of education in the country, mine is a story of chronic adversity that has resulted in PTSD. I am getting better and I am doing something about PTSD, as people tend to do when something significant enough happens to them. My books are available in libraries and bookstores and my blogs have an international following.
Even though I did everything, and accomplished and achieved everything, and succeeded at everything that those who have the money and power demanded of me and more, still I have nothing to show for it. I have been persecuted because I believe in God and try hard to follow the Ten Commandments of God in a society, culture, economy that says it believes but that does the opposite of believing in God. My story proves my persecution, which is why those who have the money and power would have me dead. Since I am still here, though, I am sharing my incredible story with you.
In retrospect, I have had PTSD for a long time, most of my life. In pictures of me, that “shell-shocked” look was often present. My high energy level and ability to work so long and hard was because my normal state was fight-or-flight mode. I am as tall as the average American man, my body-mass index (BMI) has always been at the bottom of the normal range, and my chest is almost flat. I danced ballet on pointe until working my way through college was all I could do. I figured out how to remove my ingrown and infected toenails myself.
Even though I already had pretty much every known predisposition to developing PTSD, I was not diagnosed until after I finally ended up with a nervous breakdown after a really bad emergency department visit where our “managed” health insurance made me wait in pain for 10 days to see if antibiotics would work instead of what should have been same day surgery (you can read more of the story at https://myspiritualassociation.com/2017/10/07/three-centimeter-incision/ ). Even Wikipedia has cited evidence that antibiotics do not work for a Bartholin gland cyst that has been festering for more than two decades!
The lubricant mixed with spermicide (the surfactant nonoxynol-9) on the latex condoms we had 20-30 years ago got sticky and tacky, especially when mixed with some blood and sweat and leading to many tears. Suddenly the condom got sticky and tacky enough to pull down and roll down the upper edge and bite my vagina, causing a Bartholin gland cyst. His urethra was ripped open so that it was painful to urinate for days afterwards. Sadly, most condoms are not recommended for use with oil-based intimate lubricants that do not get tacky or sticky, ever, no matter what, not even during prolonged sexual activity.
They just drained my Bartholin gland cyst the first time. It is as if they popped the zit but left the core in there to fester. The core then festered over time until the cyst got inflamed enough again to perform the marsupialization surgery. In other words, the way they left me after the first surgery, my Bartholin gland cyst had to get a lot worse again before it could get better. My vaginal gland swelled and hurt every time I became sexually aroused for the next twenty years. This was intense and relentless negative conditioning that took a severe toll on my marriage. See the film A Clockwork Orange (1971 dystopian crime film by Stanley Kubrick based on Anthony Burgess’s 1962 novel) for a violent and graphic depiction of behavior modification involving classic conditioning.
After the surgery, I was diagnosed with PTSD when I went to the pain clinic because I was still hurting immensely, especially since I have also been in several car accidents. Twice I have been hit by drunk drivers, I was hit by a car while attempting to walk across the street when I lived in Switzerland, and I have been hit hard in even more car accidents leaving me with chronic pain, an underlying neuropathy in the left upper back, and a neck so damaged that the pain clinic was recommending neck and back fusion surgery. Even worse, at the time of my diagnosis, PTSD was not an indication for Minnesota’s medical marijuana program, even though it is now.
Marijuana is a plant. It is also the safest drug. There are thousands of years of human experience with the plant documented in the literature, more than one can even read. No one has ever died from marijuana.
Marijuana has saved my life. I could only sleep for three hours a night or less for about a year after my nervous breakdown. It was a transdermal CBN patch from Mary’s Medicinals that allowed me to start sleeping more and more each night until I achieved 6 hours or even more sleep most nights. With marijuana there aren’t side-effects like with man-made drugs.
Common side effects of prescription sleeping pills such as Lunesta, Sonata, Ambien, Rozerem, Halcion may include burning or tingling in the hands, arms, feet or legs; changes in appetite; constipation; diarrhea; difficulty keeping balance; dizziness; daytime drowsiness; dry mouth or throat; gas; headache; heartburn; impairment the next day; mental slowing or problems with attention or memory; stomach pain or tenderness; uncontrollable shaking of a part of the body; unusual dreams; weakness; even sleepwalking (https://www.webmd.com/sleep-disorders/guide/understanding-the-side-effects-of-sleeping-pills#1). There can also be allergic reactions to pharmaceuticals as well as detrimental interactions with any other pharmaceuticals a person may be taking.
In Minnesota’s medical marijuana program, unadulterated plant material is not allowed. Smoking marijuana flowers, as human beings have been doing for thousands of years, is not allowed in the state of Minnesota. Minnesota is only certified for pharmaceutical grade and controlled oils and pills, which have side-effects that the plant does not.
A lawyer reported spending $2000/month on Minnesota’s medical marijuana program because that is how much he had to spend in attempt to take enough of the allowed formulations to feel any positive benefits. The side-effects of the formulations made him sick.
If you want to eat marijuana rather than smoking it, then it will take a lot more plant material to achieve similar effects, which is why it costs so much more to medicate by eating than by smoking or vaporizing marijuana. Before the effects of marijuana can be felt, chemical compounds in the plant must be activated by chemically changing them to remove a carboxyl group (decarboxylation). Eating marijuana raw, even a whole bag, will have little effect. To make edibles, the marijuana must be decarboxylated first (e.g., by simmering at a low temperature of 225°F-250°F in organic coconut oil for 6 hours to 3 days). See The Leafly Guide to Cannabis, A Handbook for the Modern Consumer, the Leafly Team, 2017, Twelve, Hachette Book Group, New York, NY, twelvebooks.com.
When consumed, the activated components of marijuana are absorbed through the digestive system rather than directly into the bloodstream, making it take longer to feel any effects. This is another reason why smoking marijuana is a popular form of consumption because effects can be felt almost immediately. Most commercially available cannabis edibles are expensive and filled with sugar and other unhealthy ingredients such as colors, flavors and preservatives formulated by chefs. And edibles fail to capture strain-specific effects and benefits.
A medical marijuana patient in Nevada can purchase an ounce of marijuana at a time, can possess up to 2.5 ounces of marijuana and can even grow their own plants. About $400/month or even less can be the difference between life and death, not to mention quality of life, for a medical marijuana patient in the state of Nevada of the U.S.A. In the state of Colorado, the prices for medical and recreational marijuana are even lower. You can grow more plants in the prairie than in the desert. The Colorado economy has been booming thanks to the marijuana business. They even make more money than planned and they fund their public schools. Everyone wants to live there, and it just keeps getting more and more crowded and competitive.
Sadly, Minnesota’s medical marijuana program will not work for PTSD because their formulations have lower THC levels. Marijuana strains known to be effective for PTSD are sativa strains (not indica), with high THC contents (20%-30%) and profiles of other cannabinoids (e.g., CBD) and terpenes conducive to treating chronic pain, depression, chronic stress or anxiety and promoting euphoria, relaxation and ease and feeling carefree.
Our bodies produce neurotransmitters called endocannabinoids (endogenous cannabinoids) that act on the same receptors as THC. The endocannabinoid system contributes to exercise-induced euphoria, the runner’s high, for example. So, it makes perfect sense that marijuana in general, and certain marijuana strains in particular, can help to retrain the brain that is unbalanced with too much traumatic stress and not enough positive experiences.
Use of marijuana can allow a splitting of consciousness or feelings of observing oneself. For example, you can be having paranoid thoughts and, at the same time, be objective about them. That makes it possible for you to actually laugh about how paranoid you’re being while you’re being so paranoid (see also the story “Big Pharma Gets Stoned” at https://myspiritualconnection.org/2018/05/24/big-pharma-gets-stoned/ ). Being able to observe yourself is key to changing how you react to what is done to you, which is why marijuana works for PTSD (see PTSD Physiology above).
Marijuana, also known as cannabis and many other names, contains about a hundred or more chemical compounds called cannabinoids that are not found in any other plant. While THC appears to be the main psychoactive component, other compounds must interact with THC in some complex way because patients who take synthetic THC alone complain that the pharmacological effects differ significantly from those achieved by eating or smoking the plant. For example, cannabichromene is a cannabinoid that is thought to promote the pain-relieving property of THC in addition to being known as a strong anti-fungal, a cytotoxic agent for malignant cells, and an antidepressant.
Different strains of marijuana are known to have vastly different effects, such as relaxed, happy, sleepy, hungry, euphoric, energetic, uplifted, focused, creative. Differences in effects produced by different strains of marijuana can be explained by differences in chemical composition of the different strains. In addition to cannabinoids, the complex essential oil of marijuana also contains chemical compounds called terpenes common in many plant families. Some terpenes present in the essential oil of marijuana are pharmacologically active and may synergize the effects of cannabinoids.
Analyzing the chemical composition of different strains of marijuana and correlating the composition with the physiological and psychological effects would be extremely interesting. For example, the expressed profiles of cannabinoids and terpenes can be measured using gas chromatography and mass spectrometry and can be correlated with biologic effects in humans and even pets. For example, the marijuana strains called Trainwreck and Jack Herer are known to be effective in treating PTSD. It would be incredibly interesting to analyze the underlying chemical compositions responsible for the effects. Knowing the chemical composition correlating with certain effects gives insights into mechanisms of action whereby the effects are produced and can also help predict which strains will be useful for which indications.
Money and privilege, rather than scientific facts and human rights, control the current power structure. Governments controlled by (big pharma) lobbying money still insist that validation of marijuana as a drug is necessary despite thousands of years of human experience! I spent years reading the literature about marijuana as part of my job working for one of the world’s largest pharmaceutical companies in Europe. In fact, I hold patents on novel synthetic compounds designed to mimic cannabinoids like THC. I was so successful that my boss took away my project and gave it to a white male scientist. My new project was to use genomics to make my boss’ experimental drug look good, even though it made the tails fall off mice. But humans do not have tails, he assured me, so it should be fine. Not surprisingly, the human phase I safety trial was prematurely shortened in duration, as I had warned before I left. I had to start over again as a postdoctoral researcher, this time at the Mayo Clinic in Minnesota.
Minnesota marijuana law is racist, designed to wrongfully imprison black men.
Minnesota marijuana law is against scientific facts.
Minnesota marijuana law is against the most basic human rights.
Minnesota marijuana law is oppression (e.g., by the medical device industry and the medical doctors and even the craft brewers who know that legalization of marijuana will rightfully impact their businesses).
Minnesota marijuana law denies children with seizures, veterans, most of the population the medicine they need.
Minnesota marijuana law encourages the opioid epidemic.
Minnesota marijuana law kills innocent people.
Minnesota marijuana law is against the people.
Minnesota marijuana law is hurting the economy.
“Minnesota nice” comes with a massive dose of passive-aggressive behavior. Minnesota’s passive-aggressive way of dealing with people is abuse that people with PTSD need marijuana to cope with. And if people with PTSD can’t handle the negative effects of people who deal with their frustrations through aggressive behavior towards others who do not deserve it, then nobody should have to be constantly subjected to such an accepted form of violence. No wonder transplants from places like California, Chicago, Colorado and Florida have already left or are trying to leave. The state of Minnesota seems to be discouraging transplants. For example, it takes more than four months to receive a driver’s license transferred from another state of the same country, while a renewed driver’s license is received in less than two weeks. “It’s a new system,” they said as they put another stamp on my temporary license that made it even less likely to be accepted anywhere.
I tell businesses that I have PTSD to try and prevent them from triggering me. It just seems to make them trigger me even more. Where is the education for how to treat people with PTSD? For example, why do American business practices have to be so exploitatively dominating whether it is an auto care or healthcare facility?
I took my PTSD diagnosis as an insult for months, and no one else believed it either. But eventually we read and learned enough to have to accept that I do have PTSD. And the people who knew me started saying, “oh, so that’s what’s wrong with you,” instead of “no, you don’t have PTSD.” Eventually I went back to the pain clinic to thank them, especially since they had shared with me how distraught they were that they could never really help anyone. I decided my label was useful to help me get better.
Instead of neck and back fusion surgery accompanied by great risk of opioid addiction, I underwent Spinal Decompression Therapy, a non-surgical alternative for disc related syndromes of the lumbar and cervical spine. Chiropractors, physical therapists, massage therapists, and herbalists all helped me immensely. I eat a healthy diet of natural whole foods and practice low-impact exercises daily such as yoga, walking, hiking, gardening and dancing. See my book, Sexiest at 50: PTSD PhD Marie (available at https://www.amazon.com/Dr-Marie-D-Kube-PhD/e/B07GTTMP1B and https://myspiritualconnection.org/2018/08/18/the-book-beat-bookstore/ and https://myspiritualassociation.com/2018/08/18/quimbys-bookstore/) for more advice about eating a healthy diet and living a healthy lifestyle.
I suffered from PTSD-induced constipation for almost three years. PTSD-induced constipation is like opioid-induced constipation. During the first two years after I was diagnosed with PTSD, I was so constipated that my anus was painfully dilated for days at a time. I strained so much and tried to induce bowel movements in every way (e.g., stool softeners, enemas, laxatives) until I had external and internal hemorrhoids, and both were bleeding. I stopped eating and I was even suicidal. I found that not eating when triggered is worse than eating, but eating the wrong thing(s) or eating too much is worse than not eating. Even when I did have a bowel movement, the feces were so large and hard that they were not flushable in any toilet and had to be thrown into the trash can.
My sister’s experience as a nurses’ aide included having to dig feces (shit) out of patients’ assholes when it was stuck in there and could not come out the normal way. This was one of the most life-saving pieces of information that she shared with me. Dig the shit out of your ass, if necessary. It is easier when wearing a nitrile examination glove on your hand with a little Vaseline on the fingers. It is also easier in a bathtub full of warm water with Epsom salts, but the cleanup can be messy.
The best way that I have found to deal with the PTSD-induced constipation is to drink more than one gallon of clean water every day, exercise and adhere to a healthy diet of real food. Let your food be your medicine and let your medicine be your food, said Hippocrates, the father of medicine. Even adhering to an incredibly disciplined diet of delicious and nutritious foods, PTSD-induced constipation can be a serious issue in the face of severe enough and/or persistent enough triggers. Herbal remedies can help a lot (see “Surviving PTSD” above).
My right Bartholin gland was so swollen for so long that my vaginal labia on the right side and the lymph node responsible for clearing the area were swollen and painful, too. When the swelling finally went down, there were numerous ingrown hairs in the vaginal labia, major and minor, and the crease in between. Some of the ingrown hairs were buried so deep for so long that they appeared to be partially degraded, and the hair follicles appeared fibrotic. All the swelling in the area may have prevented the hairs from growing out of the skin, instead becoming buried in and growing into the skin. Laser ablation surgery during the early 1990’s to remove papilloma virus from my vaginal labia left deep scars that probably also contributed to the problems. As the swelling went down and the ingrown hairs were removed, the whole area eventually cleared up.
Several scars around my mouth indicate that I was “bitch slapped” or punched in the face on the right and left sides of the mouth as well as below the mouth. Each of my canine teeth pierced through my face leaving scars above both corners of my mouth from the puncture wounds. The punch below the mouth was so hard that my four lower teeth appear to have pierced through the skin between my lower lip and chin necessitating several stitches and leaving irregular scars about an inch long. “Absorbable” sutures were apparently used that were not absorbed completely. I do not remember getting those stitches.
The sutures were incompletely and non-homogeneously broken down based on the multitude of fragments removed around the scar between my lower lip and chin. The fragments of sutures that were not absorbed caused inflammatory responses, called foreign body reactions, that lasted for decades and caused hypersensitivity leading to future suture rejections. One fragment was an incompletely dissolved knot that had a stench rotten enough to attract five flies outside within minutes. The smell is putrid like pus, a buildup of long-dead white blood cells. Following removal of the deepest pieces, there was profuse bleeding for about 30 minutes or more, enough to saturate a wash cloth.

Profuse bleeding from a small hole left after removal of a suture fragment
Removal of incomplete suture degradation products released toxins into my blood. I woke up in the middle of the night in a neck spasm that turned the right side of my neck into rock-hard knots. The large muscle going down the back and up into the right side of the neck was in total spasm. I stopped breathing twice that night. Michael woke me up. My neck was inflamed for days. I could hardly sleep or walk or sit or do anything for several days. Removal of suture pieces went on for months.
Getting punched in the face can cause pain, suffering, disfigurement, scarring, inflammation and other problems such as self-esteem problems for the rest of your life.
A fall on my lower right chin during childhood necessitated sutures and was poorly sewn up. The wound closed over, but the scar and surrounding area remained swollen and tender for decades. When I had several moles removed from my upper torso during my late forties, the sutures were rejected by my immune system and had to be removed from the inflamed and pus-filled wounds. It is likely that the sutures used to stitch the puncture wounds left after removing the moles were made of the same material as the sutures that had been used to stitch my face during childhood. Following a nervous breakdown at age 48, my chin scar became inflamed and filled with pus. Several small remnants of the sutures were removed that were left by the bone when the sutures were pulled out decades earlier. It is also possible that these stitches were “absorbable” stitches that failed to absorb.
War is responsible for my PTSD. Born in Germany in 1935 and 1940, my parents were just little children who were bombed during World War II. They survived to live in the aftermath where there was not enough food to eat and they burned their furniture to stay warm. The children played with the money like toys because it was that worthless. I blame the war for destroying my parents and my family and my life.
After the war, there was a demand for the German scientists in North America, so I was born in Canada shortly after my father finished his Ph.D. in geology and his field work in Germany and landed his first job in Saskatchewan. The next job moved us to New Mexico, USA when I was three and started to downhill ski. In 1972, when I was 5 years old, we moved to Denver, Colorado where I eventually graduated from high school in the Denver Public School system. My older sister and I were bullied relentlessly from kindergarten through high school graduation in the Denver Public Schools. Our parents wrote and spoke English well, but with a German accent, and we had German names. I finally switched my first and middle names, Dagmar Marie, during my divorce, since the bullying never stopped. We were different, so we were bullied. When we got on the bus for the 45-minute ride to our school in the ghetto downtown, all the kids chanted “Nazi, Nazi, Nazi” and the black bus driver and bus aide did nothing. The other kids would not even let us sit down anywhere.
I was beat up by a gang of Chicanas in grade school and I got a concussion. It was one of the few times I saw my only surviving grandparent as she arrived for her visit from Germany that day. I remember laying on the couch when she arrived from the airport and seeing several of her as I could not focus my eyes and didn’t know if I ever would be able to again or not.
In junior high school, I was stuck in the butt with an ice pick while waiting to enter the cafeteria for lunch. We were not allowed to go outside because it was too dangerous in the ghetto for white people, especially girls. At 15 years old, I was given alcohol to drink and raped by my teacher, and that is how I lost my virginity. At 16 years old, I started smoking cigarettes. I never got invited to a school dance, never. I couldn’t wait to graduate from high school because I believed that people would grow up and become nicer. But then my father lost his job when the oil and gas industry laid off thousands of geologists all at once.
By 18 years old, I was on my own. I lived with my boyfriend who was also my boss at the fast food restaurant where I worked. He beat me up so badly that the neighbors called the police to come and stop him. Luckily, I was able to lock myself in the bathroom until the police arrived and, once again, I survived.
Despite having significant hearing loss in one ear leading to auditory processing disorder, I paid for my bachelor’s degree in chemistry with a minor in mathematics all by myself. I earned almost straight A’s and a lot of honors along the way. I am a philosophical doctor now and I have never taken out any student loans. It took me five years instead of the usual four to earn my bachelor’s degree. I worked four or five different part-time jobs at a time, mostly as a cocktail waitress getting abused by drunk men and women. Working in restaurants kept me fed, albeit barely at times. I was so stressed out that I ground my teeth at night until my jaw hurt in the morning and the gums receded from the surfaces of my teeth leaving the nerves painfully exposed. After I graduated from college I got a “real” job and moved to another state all by myself. But first I had to have an abortion.
When I started my first real job at a pharmaceutical company in a red state, I was so abused by my boss that she eventually had to leave the company. I was the fourth underling she had destroyed and the only one who could do anything about it. I remember crying so hard on the way home from work many evenings that it was difficult to drive. I went on to develop the formulation for Humalog®, a rapid-acting insulin product still being used by diabetics today, after they demoted me from research to development. They loved all the money and careers I made for them; they just did not like my methods of honesty, integrity, transparency and true merit.
The drugging and raping did not stop until shortly before I was married at 28 years of age. I believe that drugs were mixed with my drinks and/or foods so that I would not be aware or remember the events. I was always confused when I awoke, and I felt like I had been heavily drugged because I had headaches and was hungover and violated and could not concentrate properly. I believe I was most likely drugged with flunitrazepam, also called Rohypnol, based on its known effects including impaired psychomotor function and anterograde amnesia. In fact, flunitrazepam is known to be used in drug-facilitated sexual assault.
I learned karate to defend myself at a young age in elementary school. As a young adult I later warded off one of my would-be-rapists with a shotgun. I had pet dogs most of my life to help me and protect me. I would have died of diarrhea alone in Mexico if not for the nice English teacher I met on the beach. He brought me tetracycline to take after I could no longer leave my room or even drink a glass of liquid without having diarrhea almost immediately afterwards.
I was raped by different men in different countries and sometimes more than one person at a time. One time, a lower dose of drug was used, and I could open my eyes just enough of a slit to see the shoes and ankles of the woman in whose home I was staying. I also realized that I was on a table and at least two people were having sex with my body. I saw the shoes leave the room. I couldn’t move.
A medical doctor told me that women like me who have been raped are not capable of a normal relationship. However, I was married to the love of my life for over 20 years before my nervous breakdown (you can read more of our story at https://myspiritualassociation.com/2016/09/17/mike-and-me/ ). My grandfather-in-law had fought against my people during WWII, and my mother-in-law lived with the USA occupation forces in post-war Germany when she was just a little girl. My wedding was a clash of cultures, to say the least, even though we all look similar, we all have an American passport and we all have similar socioeconomic status. We should have just eloped, but we honored our family and friends.
My husband was wrongfully injured due to sick building syndrome, which cost him his career (you can read the story at https://myspiritualassociation.com/2017/05/12/medical-mold/ ). I got sick during graduate school as well. We both still suffer consequences of our exposures to molds, chemicals, biohazards, and radioactivity in the name of science that is immoral and unethical and unbecoming of Christians.
The list of achievements necessary to become an independent researcher or, eventually, just to be able to eat, was always increasing in length and unreasonableness as the baby boomers relentlessly oppressed Generation X and reneged on every promise. It is easier for them to try and kill us than for us to complain about it. People with business degrees who know nothing about science have been put in charge by greed, and people have died and are dying because of it.
After earning my PhD degree in microbiology and immunology, I went to an ivy league school, finally, for my first temporary position as a postdoctoral researcher. But I correctly predicted that the research I witnessed there would lead to death of human gene therapy research subject(s) (you can read the story at https://myspiritualassociation.com/2017/07/13/eugenics-therapy/ ). I left there and went back to my PhD mentor’s lab. The head of my department came and threatened me and my mentor that people cannot just quit and leave a lab, let alone say such things about such a powerful and famous scientist. They thought I was crazy. But within two years, 18-year-old Jesse Gelsinger became the first person publicly identified as having died in a clinical trial for gene therapy just as I had warned.
I developed uterine fibroids that got worse and worse until my uterus was finally removed. The fibroids bled so much for at least two weeks every month that I ended up with anemia (11.8 g/dl hemoglobin when the normal range is 12-16 g/dl). No matter how many pads or tampons I used and no matter how big they were, there was always blood spilled everywhere. I woke up during my total vaginal hysterectomy on October 20, 2010 because they had to yank so hard to remove the mangled womb from my body. There were at least seven fibroids that were each 1.1 cm to 5 cm in diameter. I had a hard time waking up after the surgery, especially with the extra dose of anesthetic used to put me back under again after I awoke during the operation. I finally woke up enough only to throw up. Uterine fibroids are most likely a side effect of taking birth control pills.
I was so shamed and blamed in my life that it caused fragmentation of my personality. My coping mechanism was to split off parts of my consciousness that were aware of trauma and simply go on with my life as if nothing had happened. I feel like I became an actress out of necessity to survive, and not because I was trying to play games with people or be deceiving or dishonest in any way. I simply tried my best to be what people wanted me to be. I always said, “I’m sorry.” I never knew that people considered me beautiful and that that was one of my biggest problems. I saw that the beautiful people were popular and had an easy time getting jobs, friends, money, attention, and whatever they wanted. I was always treated poorly, exploited and taken advantage of because I am nice and “the nice guy finishes last.”
Eventually it all caught up to me. My consciousness could not be split anymore. Integration of the fragments of my consciousness has involved changes in my voice, language and even grammar. I started writing what I wanted to say instead of what employers or clients or investors wanted me to say. My two websites (www.art-and-smart.com and http://www.MySpiritualAssociation.com ) show my split personality. I use the Instructions for Helping to Improve the Human Condition (available at https://myspiritualconnection.org/instructions/ and at http://a.co/3LVufm5) to heal my fractures with help also from my spiritual advisors and shamans.
I have had a hard time finding psychologists and psychiatrists that are effective at helping me. If PTSD therapy is so effective, then why are people with PTSD killing themselves every day? And why are there so many graduates with psychology degrees? And why are so many people with psychology degrees trying to become nurses?
For example, a newly married and pregnant young woman is not an appropriate leader of a grief group for widows and widowers, regardless of what kinds of degrees or certifications she has! And the reason why Marsha Linehan is royalty in the field of psychology is because she figured out how to help herself and others like her.
So, it hurts me especially that so-called friends and family abandoned me and told my ex-husband to do the same when I needed help so that I would be forced to go to the psychologists whom they recommended. But who was going to pay those people a lot of money to talk to me? And do you really think I want to talk to someone who will only talk to me if they get paid a lot of money to do so? I do not see how someone suffering with PTSD could benefit from expensive and invalidating “talk therapy” led by someone who never had PTSD and has no idea what it is like.
It is also hard to trust psychiatrists who are testing drugs on people with PTSD when they have wrongly concluded that PTSD is primarily a mental disorder. The fact that these doctors are experimenting with humans under a false paradigm is evident by their lack of success despite ample funding and publications. To admit they are wrong would cost them their funding, careers, and livelihoods, in clear conflict of interest. An accomplished scientist like me with PTSD gets nothing while others make lucrative careers researching and treating a condition they obviously misunderstand, making them and their falsities ineffective at best and detrimental at worst. They even threatened to use drugs to erase my mind because I could not process the trauma anymore.
Supposed friends asked my ex-husband why he was helping me when no one else would. People who do not help others do not get to go to heaven. See Luke 10:29 for the good Samaritan parable about being a good person.
Love saved me. I forgive those who didn’t, for they surely knew not what they were doing. And that is why I am writing this report. And that must be why the good Lord let me get PTSD.
When I was the most hurt, heartbroken, and disabled with the stigmatized PTSD diagnosis and nowhere to go, my closest friends told me that being a waitress was the best thing for people like me. Serving food and cocktails for tips was one of four or five jobs I did at a time to pay for my undergraduate chemistry degree. I also taught organic chemistry laboratories part-time at the university. But now no one will hire me to be a waitress, or even a laboratory assistant or any job that I am overqualified for, which seems to be all of them. Not that being “overqualified” is a legitimate reason not to hire someone, especially in fields such as science and education. Yet people with only a master’s or bachelor’s degree have been getting away with “no PhDs need apply!” And when privilege overpowers merit, then people die! A career counselor advised me to “dumb down” my resume in California this summer because she has so many PhD’s already that she cannot find jobs for.
Now that I am a doctor and have dedicated my life to helping people, it hurts to be so disrespected by those closest to me whom I have even served. The emotional shocks have been sanity-defying and life-threatening. American culture has stigmatized PTSD immensely, and the ways in which the American people deal with those who have PTSD are destructive. Because people who have PTSD are not at fault and are not to blame for their condition, the disgracefully poor treatment of this population must surely be born out of ignorance and falsities propagated by the guilty and greedy warmongers who are responsible for the atrocities that cause conditions like PTSD.
The ways that Americans deal with PTSD are invalidating and make it worse and induce suppression and drive people with PTSD to suicide that is more akin to murder. Stigma protects the perpetrators and harms the victims. For example, suppression and oppression ensure that no one speaks up. And if no one speaks up, then problems like rape simply do not exist. At the time when I was first raped at 15 years old, the punishment was only a misdemeanor, and then only in the rare cases that could be proven.
American culture is competitive and materialistic, celebrating selfishness and over-indulgence. Those who are ahead are held back relentlessly instead of being nurtured. People think of themselves as Christians, but they do not really believe. They do not even follow the Ten Commandments. They say “I love you” too easily and without meaning. They “love” you like they “love” your shoes or that television show. Lying, cheating, and stealing are rewarded. Donald Trump is the President of the U.S.A.
“Social withdrawal is a hallmark of PTSD,” I read in the literature as I was preparing to write this report within weeks of erasing my Facebook account. Except for a few angels, my social network seemed less like support and respect and more like bullying and invalidation and exploitation and competition and oppression. What was in it for them? Supposed family and friends turned me away when I was fighting for my life, even after my husband and I had been there for them through thick and thin and at our own expense. I have almost used up my life savings and I am still trying to figure out how to make it, despite all my accomplishments.
People are dishonest and lie and pretend to like me and even say that they love me when in reality they have nothing but ill feelings towards me and bad thoughts about me because they are jealous, because I am German-American, because I am not fat, because I am a doctor and/or because their husbands want to have sex with me. Me not being interested in their husbands only makes it worse. Why don’t they just lose weight and work on feeling better about themselves rather than taking it all out on me just because I am nice?
PTSD is like the ultimate blunt force trauma that is not so visible from the outside, making it even more deadly. People think that if you look fine, then you should be fine and if you are not fine, then it must be your fault. Further, people seem to believe that bad things only happen to bad people. But then they must not believe in Jesus Christ, and they cannot honestly call themselves Christians!
My career ended when the CEO of the startup company I worked for paid himself with investors’ money but did not pay the people and companies who were doing the important work required by the FDA. I tried hard to get a job the first couple of years after I was laid off. Unemployment was demoralizing. I started gardening and reading more about herbal medicines and spirituality. After having been paid a lot of money in the past to write what others wanted me to say, I finally started writing more of what I wanted to say, a lot more. With Michael’s help I have now published 2 books, 2 blogs, and a magazine. Our books are available at https://www.amazon.com/Dr-Marie-D-Kube-PhD/e/B07GTTMP1B and https://myspiritualconnection.org/2018/08/18/the-book-beat-bookstore/ and https://myspiritualassociation.com/2018/08/18/quimbys-bookstore/.
For those of us with PTSD it is controversial whether to confront stressors, but I have no choice because mine are so pervasive. I would say to avoid what you can and deal with what you have to with as much support as you can get. One time I was triggered so badly when I again lost my home and had to find another place to live that I passed out completely. Other times I couldn’t walk when sufficiently triggered and I did not know if I would ever be able to walk (or dance) again. Still, I am getting better every day and I am living my life. I thank God, my ex-husband, my sister, my brother-in-law, herbalists, chiropractors, spiritual advisors, shamans and dancers for saving my life. If you cannot rely on people, then you can always rely on God (see the Instructions for Helping to Improve the Human Condition at https://myspiritualconnection.org/instructions/).
Live or Cry; Laugh or Die
The information reported here is not intended for publication in a peer-reviewed scientific journal for several reasons. First, it takes too long, and this report contains important information to save lives and reduce morbidity. Second, contributors to this work have already published results of much other scientific research in some of the world’s best scientific journals, but hardly anyone seems capable of understanding most of the information, let alone the ramifications thereof. Third, the peer-review process has been broken by conflicts of interest, greed, privilege, oppression and other such tactics unbecoming of a profession that purports to be noble. This is especially true in the case of PTSD because the same institutions that cause the problem are the ones that fund the research, education, and literature about it, in clear conflicts of interest. Contributors to this work also hold granted patents on other subjects (not just provisional patent applications that were abandoned after the one-year provisional period for lack of utility) and do not, therefore, intend to patent any of this work because they believe in truly helping people rather than making themselves rich.
Lots of Love,
Marie and Michael

The printed zine version of this blog post is now available at Quimby’s Bookstore in Chicago, Illinois, USA (www.quimbys.com)! Thanks for all your support!
LikeLike